
HOW TO MAINTAIN CQC COMPLIANCE
Regular CQC audits: How to self-assess like a pro
Regular self-audits are one of the most effective ways to understand how your service is really performing, long before an inspection takes place. Approaching it as an ongoing habit helps you spot risks early and build a more confident, resilient clinic.
 |
Gabi Ashton |
.webp?width=600&height=317&name=Regular%20CQC%20audits%20(1).webp)
When I talk to providers about auditing, I often sense the same reaction: a mixture of dread and uncertainty. Audits can feel overwhelming. Time-consuming. Another compliance task to add to an already busy clinic.
But here’s the reality: regular, meaningful self-assessment is one of the strongest protections and strengths you have for your service.
A good audit is not about ticking boxes for the Care Quality Commission, but understanding your service well enough to fix issues before they escalate and to build a culture of steady, confident improvement.
Why self-audits matter
Under the framework set by the Care Quality Commission, providers must assess, monitor and improve the quality and safety of their services. This expectation is embedded in the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014 and the Care Quality Commission (Registration) Regulations 2009.
But legislation aside, the purpose of an audit is far more practical.
An audit acts as an early warning system. It allows you to identify gaps before they become incidents and provides tangible evidence that standards are being met. It shows the team, your stakeholders and your patients that management is proactive, not reactive.
And importantly, it highlights good practice too. Audits are not just about finding faults. They often uncover strengths you may not have formally recognised. These strengths contribute directly to team confidence and professional development.
The risk of not auditing regularly is rarely dramatic at first. It’s subtle. A missing employment gap explanation. An overdue supervision. A complaint logged but not fully analysed for forward learning. Individually these seem small, but collectively they point to governance gaps.
Strong services find those gaps before regulators do.
What a good CQC self-audit actually looks like
One of the biggest misconceptions I see is that an annual audit is a single exercise completed in one sitting. A meaningful self-audit is a structured review of your entire service against CQC requirements. That takes time. It should be spread across weeks, often months, and embedded into your calendar.
If you are unsure what to audit, go back to the Fundamental Standards and the CQC’s five key questions. Your audit structure should mirror them closely. Everything you need to understand about what good care looks like is set out there.
A simple audit cycle works perfectly well:
- Identify the topic: Select a clinical practice or process for evaluation based on ongoing monitoring, priorities or identified risks.
- Define standards: Define clear, evidence-based standards and criteria against which performance will be measured.
- Collect and analyse your data: Gather data to assess current practice against the predefined standards and use it to identify any deviations from the set standards.
- Implement changes: Develop and apply strategies for improvement based on the data analysis.
- Re-audit: Repeat the audit after a set period to evaluate the effectiveness of implemented changes and ensure continuous improvement.
It does not need to be complicated, but it needs to be complete.
A practical way to think about auditing:
The 3 P’s
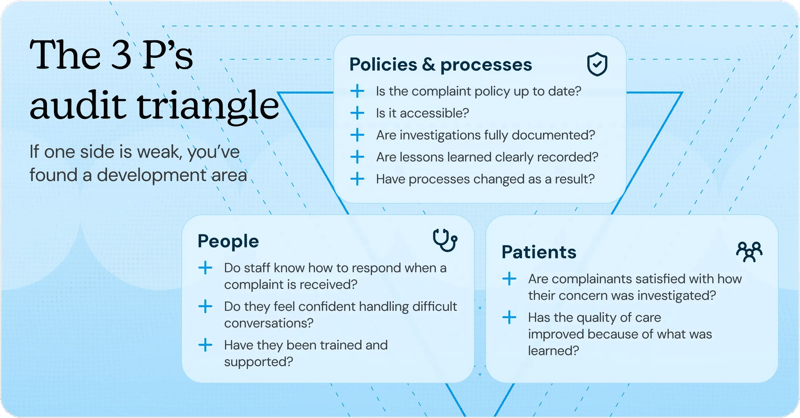
With my experience in CQC, I’ve found there’s one model that consistently prevents blind spots: thinking in terms of Policies and Processes, People and Patients.
For every audit topic, you should be able to draw a full triangle between these three areas.
Let’s take complaints as an example. First, consider your policies and processes. Is the complaint policy up to date? Is it accessible? Are investigations fully documented? Are lessons learned clearly recorded and have processes changed as a result?
Second, consider your people. Do staff know how to respond when a complaint is received? Do they feel confident handling difficult conversations? Have they been trained and supported?
Third, consider your patients. Are complainants satisfied with how their concern was investigated? Has the quality of care improved as a result of what was learned?
If you can confidently connect all three points, you are auditing thoroughly. If one side of the triangle is weak, you have identified a development area.
The crucial evidence clinics commonly miss
When reviewing documentation, certain gaps can appear repeatedly.
Full employment history can be incomplete with unexplained gaps. Supervisions and appraisals may be overdue or poorly documented. Consideration of Duty of Candour (being open and transparent with people who use your service) following learning events may not be clearly evidenced. Regulatory notifications (requirements to report deaths of service users, serious injuries, allegations of abuse and events impacting service safety) may not have been fully considered.
These are rarely deliberate omissions. They are usually a symptom of not stepping back to review the whole picture.
Evidence storage does not need to be sophisticated. You don’t need complex software. What you need is one secure, organised central location where information is stored logically, with appropriate access controls. Governance documents may be widely accessible; recruitment files should not.
Turning audit findings into meaningful improvement
When gaps are identified, the way you respond matters. Bring the team together. Explore what happened, when, why, where and how. Resist the temptation to focus on who.
As the Registered Provider or Registered Manager, you hold legal accountability for governance. Delegation is appropriate, but oversight remains your responsibility. It is not enough to say, “My Practice Manager handles that.” You must be confident that it is being done well.
Prioritise issues based on seriousness, potential impact on people using the service and how many individuals are affected. Develop clear action plans with named responsibility and deadlines. Monitor progress consistently. And then measure impact: Are the changes working in practice? Are they sustainable?
Some improvements can be re-audited quickly. Others may take months to show measurable impact. The subject matter and the findings should determine the timeline.
Common audit mistakes

One of the most common mistakes I see is this: auditing without review. Audits may be completed, but if they’re superficial or poorly aligned to standards, they offer false reassurance.
This is one area I always advise providers to audit first: audit your audits.
There’s an old Latin phrase that roughly translates to: ‘Who’s watching the watchmen?’ In your audits, you may delegate parts of assurance to your team, but as the Registered Manager or Provider you remain accountable, so you need confidence that audits are robust, consistent and followed through.
So, review a sample. Are the conclusions robust? Are the standards clearly defined? Are actions followed through? More often than not, reviewing completed audits uncovers deeper conversations about teamwork, competency, risk awareness and leadership support.
Making auditing part of your company culture
The strongest services don’t see CQC compliance as ‘them and us.’ They integrate the Fundamental Standards into everyday language and behaviour.
If a complaint is received, don’t react in silo. Thank the patient, investigate thoroughly and be open and honest about what you’ve learned. Share those lessons learned with your team and support them through the review process. Consider whether regulatory notifications are required.
In doing so, you are naturally demonstrating compliance with multiple CQC regulations, not because you’re performing for inspection, but because you’re leading well.
If you want your team to deliver high-quality care and remain engaged with compliance, you must model that commitment yourself. Delegate based on interests, passion and professional development where possible. This empowers staff and shifts auditing from reactive stress to proactive pride.
Learn more about building a culture of continued excellence.
Preparing confidently for future inspections
Regular self-auditing builds confidence. When inspection time comes, well-audited services are not scrambling to gather evidence. They understand their strengths. They know their development areas. They can demonstrate learning and improvement clearly.
Inspectors notice when a service uses everyday experiences, such as complaints, incidents and feedback, as opportunities to improve.
Good governance is a golden thread. When woven consistently through daily practice, it becomes visible in every conversation, document and decision.
Keep your audit schedule short, simple and regular. Identify learning events early. Act steadily. Revisit impact.
Do that and you will not only meet regulatory expectations, you’ll build a service that is genuinely safer, stronger and more resilient over time.
Top 4 self-audit tips for small clinics
- Develop an audit schedule from day one. This could build in weekly, monthly, quarterly, annual audits that cover all topics and ensure you are well covered.
- Don’t overthink what it is you need to audit; when in doubt, use the ‘Fundamental Standards’ as a prompt.
- Keep your audits in one central space; it’ll help you see emerging patterns.
- Always make sure any audit findings are appropriately aligned with asking yourself: Is this a CQC notification under the Care Quality Commission (Registration) Regulations 2009?
.webp?width=800&height=240&name=Article%20Image%20-%20Bio%20G%20(1).webp)
Gabi Ashton has worked in the Health and Social Care sector for over 15 years, in CQC-regulated services and as a CQC inspector. Her experience on both sides of CQC has given Gabi valuable insights into why and how services are rated from Inadequate to Outstanding.
Gabi now runs Let’s Make Lemonade, specialising in CQC compliance with the aim of driving improvements for providers across the health and social care sector.
.webp?width=380&height=201&name=Ongoing%20requirements%20(1).webp)
.webp?width=380&height=201&name=Building%20a%20culture%20(2).webp)

